How To: JVP
It was great to receive a refresher on how to do the JVP examination during my rotation. We all know how to do the basic steps, but breaking each step down even further helped me better understand how the JVP is used and what it can tell us.
One: Identify the JVP
In comparison to the carotid pulse, the JVP can be distinguished by six unique features.
Location is between the two heads of the sternocleidomastoid muscles
Multiphasic waveform
Not palpable
Occludable
Changes with position and respiration - decrease with respiration
Changes with abdominojugular reflux maneuver
Two: Absolute Height
A normal JVP is <4cm. An elevated JVP is suggestive of volume overload, but more specifically, poor RV compliance.
Three: Abdominojugular Reflux
This maneuver is performed by applying 20-30mmHg of pressure to the patient’s abdomen. A normal response is an elevation of the JVP 2-4cm above the baseline level, and return to baseline within 10 seconds. A 2cm (70% specificity)/4cm (90% specificity) AND sustained elevation >10 seconds are required for a positive AJR exam.
Four: Waveform Analysis
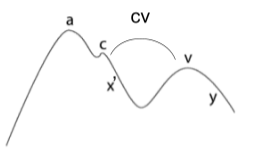
Ascent
a: atrial contraction
c: bulging of tricuspid with ventricular contraction
v: passive atrial filling
cv: specific for tricuspid regurgitation
Descent
x’: downward movement of tricuspid with ventricular contraction
y: atrial emptying with opening of tricuspid
No comments:
Post a Comment